![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
|
Advanced Imaging of the Diabetic Foot and Its
Complications
|
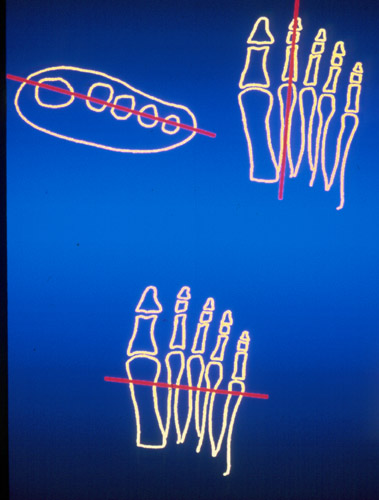
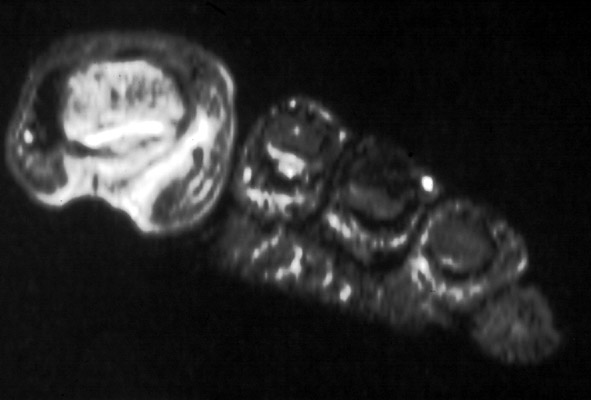
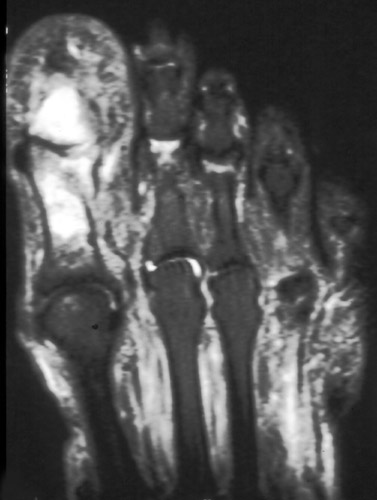
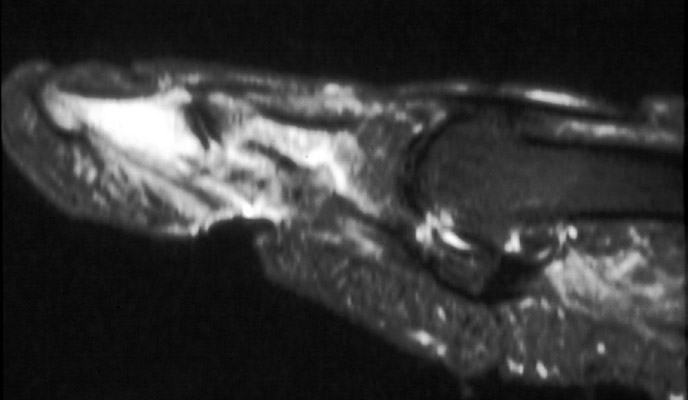
Magnetic Resonance ImagingMR imaging is the most sensitive and specific test for osteomyelitis. On MR imaging, high signal intensity in the bone marrow on T2 weighted images is consistent with osteomyelitis. Localized high signal intensity in the soft tissues on T2 weighted images is consistent with soft tissue abscess. Low signal intensity in the bone marrow on both T1 and T2 weighted images is consistent with neuropatic osteoarthropathy. False positive exams can be seen with trauma and fractures, with osteonecrosis, and occasionally with neuropathic joints. MRI PROTOCOLIMAGING THE FOOT The diabetic foot should be imaged in three planes: axial, sagittal, and coronal. Due to the confusion of labeling the cardinal planes in the foot, axial may be referred to as long axis, and coronal may be referred to as short axis. To optimize imaging, large fields of view should be avoided. The study should be tailored to the individual needs of the patient. The foot should be visually examined with bandages and wrappings removed. Since osteomyelitis occurs next to ulcers, these areas should be clearly identified and imaged. Markers are placed over shallow ulcers that may be difficult to appreciate on images. The field of view is selected that covers the areas of concern. In general, the forefoot and midfoot area are covered for evaluation of infected toes or ulcers of the ball of the foot. The hindfoot, ankle, and midfoot are covered for ulcers involving the calcaneus. Large fields of view should be avoided so that adequate detail and visualization is obtained for even the smallest phalanges of the toes.
In cases of alignment deformities, the technologist orients the slices to optimize imaging of the area of concern. For example, in cases of hallux valgus, if the 1st toe is evaluated for osteomyelitis, sagittal slices are oriented along the the 1st phalanges. If the concern is more proximal, sagittal slices would be planned along the 1st metatarsal. SEQUENCE CHOICEST1 Anatomically detailed with high resolution. Sensitive for bone marrow changes, however may miss bone marrow edema in the smaller phalanges. T2 Less sensitive to bone marrow edema, especially when fast spin echo sequences are employed due the bright signal of edema blending with the bright signal of the fatty bone marrow. T2 with fat saturation avoids this problem, but the foot may difficult to obtain a uniform fat saturation. Inhomogeneous fat saturation may lead to diagnostic error. STIR Very sensitive to bone marrow edema changes. Uniform fat saturation easily obtained. Intavenous gadolinium is generally not needed on a routine basis. It may improve sensitivity for small abscesses or sinus tracts.
Table 4. MR Imaging of Osteomyelitis
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Advanced Imaging of the Diabetic Foot and Its
Complications
>
|