Calcium
pyrophosphate dihydrate (CPPD) crystal deposition disease is slightly
more prevalent in men. Chondrocalcinosis results with deposition of CPPD crystals
in cartilage. The clinical term pseudogout represents symptomatic acute attacks
which present in a similar fashion as gouty or infectious arthritic attacks.
CPPD disease is associated with certain metabolic disorders such as hyperparathyroidism,
hemochromatosis, hypothyroidism, hypomagnesemia, and hypophosphatsia.
Calcium
pyrophosphate dihydrate (CPPD) crystal deposition disease is slightly
more prevalent in men. Chondrocalcinosis results with deposition of CPPD crystals
in cartilage. The clinical term pseudogout represents symptomatic acute attacks
which present in a similar fashion as gouty or infectious arthritic attacks.
CPPD disease is associated with certain metabolic disorders such as hyperparathyroidism,
hemochromatosis, hypothyroidism, hypomagnesemia, and hypophosphatsia.
Distribution:
The most commonly affected area of the wrist is at the articulation of the
distal radius and proximal carpal row. There is a strong propensity of CPPD
crystal deposition disease for the 2nd and 3rd metacarpophalangeal joints.
Changes at the interphalangeal joints and other metacarpophalangeal articulations
occur much less frequently and to a much lesser degree
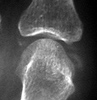
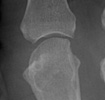
Radiographic Appearance:
Calcium deposition is often seen at the triangular fibrocartilage of the wrist.
Subchondral sclerosis, joint space narrowing, subchondral cyst formations
which may be quite large, and intraarticular bodies from subchondral osseous
collapse and fragmentation are all findings which can be seen in patient's
with CPPD disease. These radiographic abnormalities are most common at the
radiocarpal articulation and at the 2nd and 3rd metacarpophalangeal joints.
Additionally, there may a shift in the normal alignment of the scaphoid and
lunate and narrowing at the midcarpal compartment.
Differential Diagnosis:
CPPD disease causes destruction of cartilage which can lead to radiographic
findings similar to osteoarthritis. Sites of involvement are useful for differentiating
the two since the radiocarpal compartment of the wrist is not a common location
for osteoarthritis. Lack of an erosive process at the MCP joint differentiates
CPPD crystal deposition disease from rheumatoid arthritis. Greater propensity
for the MCP joints (also commonly includes the 4th and the 5th) with medial
beak-like osteophytosis at the metacarpal heads and more widespread involvement
of the carpal bones may help to differentiate hemochromatosis from idiopathic
CPPD disease.