![]()
![]()
![]()
![]()
![]()
![]()
![]()
|
|
|
INFECTION
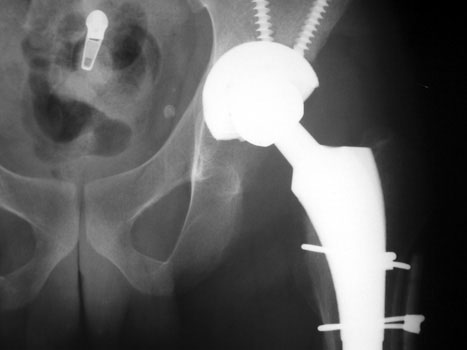
INFECTION—Markedly widened interfaces about acetabular and femoral components
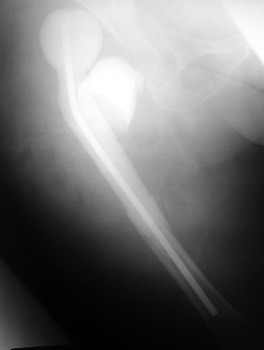
INFECTION Progressive interface widening about acetabular component
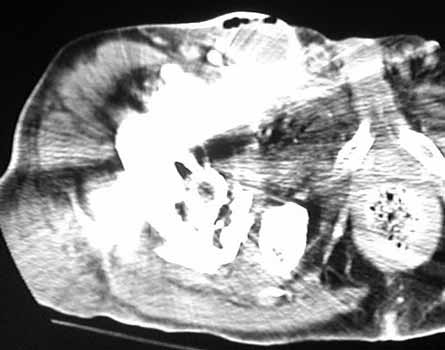
INFECTION—Soft tissue gas. Gas in neo capsule of right total hip replacement secondary to sinus tract from joint to skin
INFECTION—Soft tissue gas adjacent to dislocated cement spacer
INFECTION—Gas bubbles in synovial cyst anterior to right total hip replacement. Patient had infected left hip joint 1 year previously treated by Girdlestone procedure. Right total hip replacement was grossly loose and with migrated hardware.
INFECTION
INFECTION
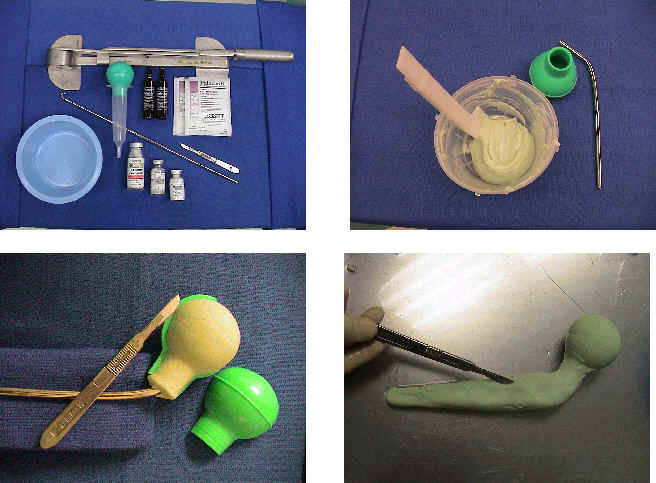
Cement spacers are antibiotic impregnated, allowing for local dispersal of antibiotics.
Cement spacers are fabricated in the surgical suite using methylmethacralate cement impregnated with antibiotics sensitive to cultured organisms. A Rush rod is cut and bent to 120 degrees to mimic the femoral neck-shaft angle. Antibiotic impregnated cement is placed into a blue bulb syringe which simulates the femoral head contour and allowed to dry. The plastic is then removed. A second batch of cement is prepared and formed around the femoral shaft portion of the Rush rod. |
|
|